World TB Day: Mots’elisi’s Story

World TB Day: Mots’elisi’s Story
Posted March 24, 2024.
 Normally based in Saskatoon, PIH Canada Board member Dr. Ryan Meili is a family physician and lifelong advocate for healthy public policy with a focus on health equity. In the article series “A View from Lesotho,” Dr. Meili will be sharing his thoughts and experiences from Lesotho, where he is currently serving as a clinical volunteer with Partners In Health, based in Maseru at Botšabelo Hospital, along with his wife Mahli, a pediatrician.
Normally based in Saskatoon, PIH Canada Board member Dr. Ryan Meili is a family physician and lifelong advocate for healthy public policy with a focus on health equity. In the article series “A View from Lesotho,” Dr. Meili will be sharing his thoughts and experiences from Lesotho, where he is currently serving as a clinical volunteer with Partners In Health, based in Maseru at Botšabelo Hospital, along with his wife Mahli, a pediatrician.
Ryan wrote this blog in recognition of World TB Day on March 24.
All photos by Josh Berson, except as noted.
Love and Consolation
 ‘Mme ‘Malerato (lerato means love, ‘Malerato, mother of love) has made the trek from her house to visit Mots’elisi twice a day for the last six months. It’s only about a twenty-minute walk, but the dirt paths through the hills of Qacha’s Nek, Lesotho, can turn treacherous in the rain and snow. Still, ‘Mme has never missed a day, she takes her job too seriously. She is Mots’elisi’s “treatment supporter”, hired by PIH to accompany her from the beginning of her care for multidrug-resistant tuberculosis (MDR-TB) to the end.
‘Mme ‘Malerato (lerato means love, ‘Malerato, mother of love) has made the trek from her house to visit Mots’elisi twice a day for the last six months. It’s only about a twenty-minute walk, but the dirt paths through the hills of Qacha’s Nek, Lesotho, can turn treacherous in the rain and snow. Still, ‘Mme has never missed a day, she takes her job too seriously. She is Mots’elisi’s “treatment supporter”, hired by PIH to accompany her from the beginning of her care for multidrug-resistant tuberculosis (MDR-TB) to the end.

Mots’elisi (whose name means consolation) is twenty-five. She usually lives with her mom, her brother and her two-year-old son Hlalele, but she has been staying on her own in a small house nearby since was diagnosed with MDR-TB last July. This new illness came about six months after she’d been diagnosed with HIV and started anti-retroviral therapy. “I noticed I was losing weight,” she told me, “and then I started to cough up blood.” She figured it was TB because these were the same symptoms she’d had ten years earlier when she’d been treated for drug-sensitive TB.
At the hospital, she provided a sputum sample. A GeneXpert PCR test was positive for Mycobacterium tuberculosis, the bacteria that causes TB disease. This time, the bug was resistant to rifampin, one of the key drugs for treating tuberculosis. This meant her TB couldn’t be treated with the regular drugs, and she would need to be enrolled in the MDR-TB program. She is not alone in this diagnosis. TB affects a quarter of the world’s population, with MDR-TB accounting for 3.5% of new cases and 18% of cases among people previously treated for TB. Lesotho has the highest per capita rate of TB in the world, major challenges in diagnosis and treatment, and a high burden of MDR-TB.
The care of MDR-TB is challenging, and for patients like Mots’elisi it takes a team.

Partners In Health Lesotho supports three main activities: the Rural Initiative (RI), establishing primary care in remote communities; Health Systems Strengthening, supporting the Ministry of Health in developing the 5S’s as PIH calls them (staff, stuff, space, systems, social support; and MDR-TB, delivering care in Lesotho also in partnership with the Ministry of Health).

Most of the work is on the ground but some of it very high level. Lesotho is the highest country in the world, tiny but geographically challenging. Many of the communities we serve are accessible only by rocky mountain trails, and occasionally by helicopter or small plane. Here Mahli (second from left) joins PIH Lesotho Executive Director Dr. Melino Ndayizigiye (far left), Clinical Director Dr. Afom Andom (second from right), and US emergency physician Dr. Chanel Fischetti (far right) for a tour of rural sites.
Dr. Melino demonstrates the use of POCUS (point-of-care ultrasound) at the partner Senkatana oncology centre next to the MDR-TB hospital.
 Dr. Melino demonstrates the use of POCUS (point-of-care ultrasound) at the partner Senkatana oncology centre next to the MDR-TB hospital.
Dr. Melino demonstrates the use of POCUS (point-of-care ultrasound) at the partner Senkatana oncology centre next to the MDR-TB hospital.


The first step in MDR-TB treatment is diagnosis. Ntate Rethabile and his team at Botšabelo Hospital’s lab utilize GeneXpert PCR to diagnose TB and determine its drug resistance, alongside monitoring other key lab findings such as CD4 counts and viral loads for approximately three-quarters of MDR-TB patients who are also living with HIV.
Some patients are ill enough at diagnosis or later in treatment to require admission to Botšabelo MDR-TB Hospital, where they are cared for by a multidisciplinary team including nurses, ward attendants, x-ray technicians, mental health counselors, cleaners, administrative and logistical leaders, as well as medical professionals including general practitioners, internists, a critical care specialist, a pediatrician, an infectious disease specialist, and a radiologist.

Most of the patients are adults, like Mme Selloane, here being examined by Dr Ninza, a critical care specialist from Zambia. Selloane has been in and out of hospital due to complications of her care, with added challenges as she lives two hours by horse from the highway. Fortunately, after months of treatment and observation, she’s now back home and doing well.

We do see the occasional child, like my friend Tlotla who came with us from one of the mountain communities to be seen and have his treatment started in hospital.

The sickest of the patients are seen in the ICU, where the team provides high quality care, consistent with the philosophy of PIH that everyone deserves to benefit from the best of scientific advances. PIH promotes the notion of a “preferential option for the poor” in its medical services, believing that people shouldn’t be denied good care because they live in poverty, and that those most in need deserve the most help.

Ntate Thulo and the pharmacy team prepare the medications, including the highly specialized MDR-TB drugs, for the inpatients and for the bulk of the MDR patients who are seen in the community.

As part of the MDR-TB program, PIH also operates rotating community clinics in nine of the country’s ten districts. Here Mme Mpho, a member of the community nursing team, prepares the files, making sure everyone’s labs and meds are up-to-date.

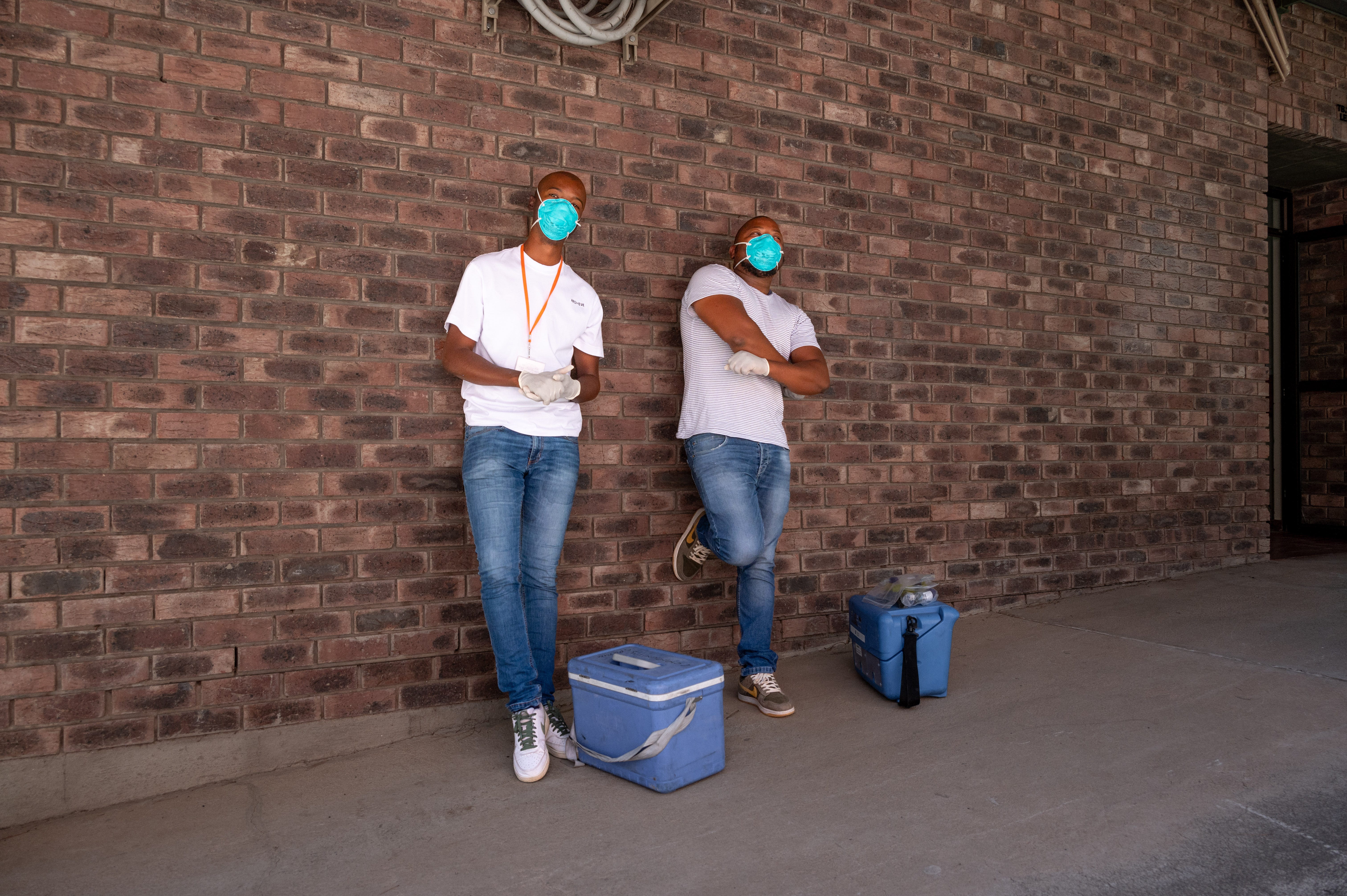
 Loaded up and ready to go, the PIH team is ready to head out to the district health centres.
Loaded up and ready to go, the PIH team is ready to head out to the district health centres.

 The roads are long, switchbacked, and frequently treacherous in the high mountains.
The roads are long, switchbacked, and frequently treacherous in the high mountains.

But we’re in good hands with drivers like Ntate Matlosa who has a keen eye for potholes and crossing sheep and cows.
 Here we see community nurses Lebitsa and Ntsapi looking badass enough to tackle any mycobacterium.
Here we see community nurses Lebitsa and Ntsapi looking badass enough to tackle any mycobacterium.
Each outreach team consists of a doc, driver and two community nurses. When we get to clinic, we unload the files, medications and food packages, then start seeing patients.
 This is where we meet Mots’elisi, at Machabeng Hospital in Qacha’s Nek. After listening to her lungs and heart, reviewing her chest x-ray and renewing her prescriptions…
This is where we meet Mots’elisi, at Machabeng Hospital in Qacha’s Nek. After listening to her lungs and heart, reviewing her chest x-ray and renewing her prescriptions…

…we went to visit her in her home. One of the key beliefs of PIH is the importance of accompaniment, of walking alongside our patients. I wanted to know more about her experience with MDR-TB and particularly with the PIH team.
And it’s a big team. She would only know the people she was directly in contact with, like our group that had come out for clinic, but there are over 450 staff and over 125 treatment supporters working for PIH in Lesotho.
Undergoing a treatment that involves taking medications daily for six to eighteen months is not easy. The illness itself, medication side effects, and the near constant underlying poverty and food insecurity make it even harder. This explains why as few as 70% of MDR-TB patients successfully finish their treatment.
 As for ‘Mme, she has accompanied several patients over the years. She receives payment for her work, and with a new baby at home, the money coming in goes a long way. She also appreciates the chance to make a difference. “I know that when I go to see the patients, I’m able to help them understand and motivate them to take their medications.”
As for ‘Mme, she has accompanied several patients over the years. She receives payment for her work, and with a new baby at home, the money coming in goes a long way. She also appreciates the chance to make a difference. “I know that when I go to see the patients, I’m able to help them understand and motivate them to take their medications.”
This accompaniment model is central to PIH’s vision of care. The organization believes in paying local health workers and in providing for more than just the immediate medical needs of the patient. PIH’s connection to community allows them to build the team that can deliver that care.

It’s not an easy time for Mots’elisi –completing MDR-TB treatment is hard work – but she’s going to be ok. Thanks to the care of people like ‘Mme ‘Malerato, community connections become personal connections. Those connections help patients like Mots’elisi feel loved and valued, and ultimately to be cared for and cured.



